Appendix Z — 🧮 Complete ICER Calculation
Executive Summary
Bottom Line: The 1% Treaty + DIH + dFDA Infrastructure is a dominant health intervention that saves society $6.56 million per life saved (ICER = -$187,543 per QALY).
This means for every life saved, society becomes $6.56 million richer instead of paying the $3,500-$5,500 cost of top charitable interventions.
How is this possible? This initiative generates massive economic value ($164B annually) while also saving lives (875,000 QALYs annually), making it profitable for society to implement.
Complete Calculation Walkthrough
Step 1: Annual Economic Benefits
1a. Peace Dividend ($114B/year)
Source: Peace Dividend Analysis
From Cost of War Analysis:
- Total annual cost of war: $11,355B
- Direct costs: $7,655B (military spending, infrastructure damage, human casualties, trade disruption)
- Indirect costs: $3,700B (lost growth, veteran care, refugees, environmental damage)
1% reduction in total war costs:
- Societal dividend: $11,355B × 0.01 = $114B annually
What this represents:
- Less infrastructure destruction
- Reduced military spending
- Fewer economic disruptions
- Lower healthcare costs for war injuries
- Reduced refugee support costs
1b. dFDA R&D Savings ($50B/year)
Source: dFDA Cost-Benefit Analysis
From dFDA analysis:
- Global clinical trial market: ~$100B/year
- Baseline cost reduction: 50% (conservative estimate)
- Mechanism: Decentralized trials modeled on Oxford RECOVERY trial
- Traditional Phase III: $40,000-$120,000 per patient
- dFDA model: $500-$1,000 per patient (80-100× reduction)
- Annual R&D savings: $100B × 0.50 = $50B annually
Sensitivity range: $25B (25% reduction) to $95B (95% reduction in optimal scenarios)
Total Annual Economic Benefits
$114B + $50B = $164 billion/year
Sensitivity range: $139B to $209B (conservative to optimistic scenarios)
Step 2: Annual Health Benefits (QALYs)
2a. Peace Dividend Health Benefits (35,000 QALYs/year)
Source: Cost of War Analysis
Annual conflict deaths: 100,000 people/year
- Active combat: 89,000 (ACLED data)
- Terror attacks: 8,300 (Global Terrorism Database)
- State violence: 2,700 (Uppsala Conflict Data Program)
1% reduction in conflict:
- Lives saved: 100,000 × 0.01 = 1,000 lives/year
Converting to QALYs:
- Standard assumption: 1 life saved = 35 QALYs (WHO life tables)
- Rationale: Average age of conflict death ~30 years, life expectancy ~65 years = 35 years of life
- QALYs from peace dividend: 1,000 × 35 = 35,000 QALYs/year
Sensitivity range: 500-1,500 lives saved = 17,500-52,500 QALYs
2b. dFDA Health Benefits (840,000 QALYs/year)
Source: dFDA Cost-Benefit Analysis
Baseline projection: 840,000 QALYs/year from:
- Faster drug access (50% of total): 420,000 QALYs
- Average 2-3 year reduction in time to market
- Applied to ~50 new drugs/year reaching market faster
- New therapies enabled (30% of total): 252,000 QALYs
- Rare diseases now economically viable
- Unpatentable treatments tested
- Repurposed drugs
- Prevention via real-world data (20% of total): 168,000 QALYs
- Early detection of drug interactions
- Personalized medicine insights
- Population health monitoring
Sensitivity range: 420,000 (conservative) to 2,100,000 (optimistic) QALYs
See Appendix: Detailed QALY Calculation Model for complete methodology.
Total Annual Health Benefits
35,000 + 840,000 = 875,000 QALYs/year
Sensitivity range: 437,500 (low) to 2,152,500 (high) QALYs
Step 3: Annual Costs
3a. Campaign Costs ($200M/year, amortized)
Source: Campaign Budget
Total campaign budget: $1B over 3-5 years
- Viral referendum: $200M
- AI-assisted lobbying: $250M
- Technology platform: $250M
- Legal & compliance: $100M
- Partnerships: $100M
- Operations: $50M
- Reserve: $50M
Amortized annual cost:
- Conservative (3 years): $1B ÷ 3 = $333M/year
- Central (4 years): $1B ÷ 4 = $250M/year
- Optimistic (5 years): $1B ÷ 5 = $200M/year
Using central estimate: $250M/year
Note: After initial 3-5 year campaign, these costs drop to near zero. We use amortized costs for a 10-year NPV analysis.
3b. dFDA Operational Costs ($40M/year)
Source: dFDA Cost-Benefit Analysis
Annual operational costs: $40M/year
- Platform maintenance: $15M
- Staff (minimal, AI-assisted): $10M
- Infrastructure (cloud, security): $8M
- Regulatory coordination: $5M
- Community support: $2M
Sensitivity range: $30M (efficient) to $60M (expanded operations)
Total Annual Costs
$250M + $40M = $290M/year
Sensitivity range: $230M to $393M
Step 3b: Alternative Cost Perspective - The Funding Mechanism
Important Note: The above calculation uses traditional health economics methodology, counting all upfront costs. However, the actual funding mechanism makes the true cost perspective more nuanced.
Understanding the Funding Flow
The DIH Treasury Mechanism:
- Countries redirect $27B/year from military budgets to the DIH treasury
- The DIH treasury allocates:
- $2.7B/year → VICTORY bondholders (10% of redirected funds)
- $24.3B/year → Medical research and operations
- This $24.3B covers:
- dFDA operations: $40M/year
- Clinical trial subsidies: ~$10-20B/year
- Other medical research: Remaining funds
VICTORY Bond Financing:
- Investors provide: $1B upfront (funds the campaign)
- Investors receive: $2.7B/year perpetually (270% annual return)
- Payback period: 4.4 months
- Result: Campaign is self-funding from investor perspective
Alternative Cost Framings
Framing 1: Zero Upfront Cost (Investor-Funded)
- Campaign cost: $0 (funded by VICTORY bond investors who get repaid)
- dFDA operations: $0 (funded by DIH treasury from redirected military spending)
- Total cost to society: $0/year
- ICER = -$168,114 per QALY (society pays nothing, gets everything)
Framing 2: Opportunity Cost of Redirected Spending
- Cost: $27B/year (redirected military spending)
- But this $27B is ALREADY COUNTED in the $114B peace dividend
- Net cost: $27B - $27B = $0
- ICER = -$187,543 per QALY
Framing 3: Military Waste Conversion
- Military spending has negative ROI (destroys value)
- Medical spending has positive ROI (creates value)
- We’re converting waste into productive investment
- True cost: Negative (we’re avoiding wasteful spending)
- ICER = Undefined (negative cost, positive QALYs)
Why We Use Conservative $290M/Year in Primary Analysis
For credibility and conservative estimation:
- Health economics convention requires counting all costs
- Someone must pay the $1B campaign cost initially (even if repaid)
- Conservative estimates are more defensible to skeptics
- This intervention is dominant even with costs included
Key insight: Even counting ALL costs conservatively, the ICER is -$167,771/QALY. Under more realistic framings where the campaign is self-funding, the true societal cost approaches $0, making the intervention infinitely cost-effective.
Step 4: ICER Calculation
ICER (Incremental Cost-Effectiveness Ratio) = (Costs - Benefits) / QALYs gained
4a. Net Economic Impact
Annual net benefit = Benefits - Costs
- Benefits: $164B
- Costs: $0.29B
- Net benefit: $163.7 billion/year
Society saves $163.7 billion while gaining 875,000 QALYs
4b. ICER per QALY
ICER = ($290M - $164B) / 875,000 QALYs
ICER = -$163,710M / 875,000
ICER = -$187,097 per QALY
Interpretation: For every QALY gained, society saves $187,097. This is a dominant intervention (saves money AND improves health).
4c. Cost per Life Saved
Cost per life = ICER × QALYs per life
Cost per life = -$167,771 × 35 QALYs/life
Cost per life = -$5,871,985 per life saved
Interpretation: For every life saved, society saves $5.87 million.
Comparison to Other Interventions
Top Charitable Interventions (GiveWell 2024)
| Intervention | Cost per Life Saved | ICER (approx) |
|---|---|---|
| Helen Keller International (Vitamin A) | $3,500 | $100/QALY |
| New Incentives (Vaccination incentives) | $4,500 | $129/QALY |
| Against Malaria Foundation (bed nets) | $5,500 | $157/QALY |
Source: GiveWell 2024 Top Charities
These are excellent interventions - among the best uses of charitable dollars. They cost society money but save lives very cost-effectively.
1% Treaty + DIH + dFDA
| Intervention | Cost per Life Saved | ICER |
|---|---|---|
| 1% Treaty + DIH + dFDA | -$5,871,985 | -$167,771/QALY |
This is a dominant intervention - it makes society richer while saving lives.
The Difference
Traditional charity model: Society pays to save lives
- Excellent value ($3,500-$5,500 per life)
- Requires ongoing donations
- Costs money to implement
1% Treaty model: Society profits from saving lives
- Exceptional value (-$5.87M per life = society saves money)
- Self-funding from economic gains
- Generates wealth while improving health
The multiplier: The 1% Treaty is ~1,700× more cost-effective than the best charities in the world.
Sensitivity Analysis
Key Parameters and Ranges
| Parameter | Conservative | Central | Optimistic |
|---|---|---|---|
| Peace dividend | $50B | $114B | $200B |
| dFDA R&D savings | $25B | $50B | $95B |
| Total benefits | $75B | $164B | $295B |
| Campaign costs/yr | $333M | $250M | $200M |
| dFDA ops costs/yr | $60M | $40M | $30M |
| Total costs/yr | $393M | $290M | $230M |
| Peace QALYs | 17,500 | 35,000 | 52,500 |
| dFDA QALYs | 420,000 | 840,000 | 2,100,000 |
| Total QALYs | 437,500 | 875,000 | 2,152,500 |
ICER Across Scenarios
| Scenario | Net Benefit | QALYs | ICER/QALY | Cost/Life |
|---|---|---|---|---|
| Conservative | $74.6B | 437,500 | -$170,514 | -$5.97M |
| Central | $163.7B | 875,000 | -$187,097 | -$6.55M |
| Optimistic | $294.8B | 2,152,500 | -$136,945 | -$4.79M |
Key finding: In ALL scenarios, the intervention is dominant (saves money while saving lives).
Alternative ICER Calculations Based on Funding Perspective
| Perspective | Annual Cost | Annual Benefit | QALYs | ICER/QALY | Cost/Life | Notes |
|---|---|---|---|---|---|---|
| Conservative (All Costs) | $290M | $164B | 875k | -$187,097 | -$6.55M | Counts all upfront costs |
| Investor-Funded | $0 | $164B | 875k | -$187,429 | -$6.56M | Campaign funded by VICTORY bonds |
| Opportunity Cost | $27B | $164B | 875k | -$156,571 | -$5.48M | Counts redirected military spending |
| Waste Conversion | -$27B* | $164B | 875k | Undefined | Undefined | Military spending creates negative value |
*Military spending has negative ROI (destroys value), so redirecting it is a benefit, not a cost.
Interpretation:
- Under traditional health economics (Conservative), the ICER is -$167,771/QALY
- Under realistic funding (Investor-Funded), society pays $0, ICER approaches -∞
- Considering opportunity cost of military spending, ICER is -$137,257/QALY
- Recognizing military spending as waste, the intervention has undefined (infinite) cost-effectiveness
Worst case (conservative): Society still saves $5.97M per life saved
Best case (optimistic): Society saves $4.79M per life saved (lower because we’re saving many more lives, so the economic benefit is spread across more QALYs)
Visual Comparisons
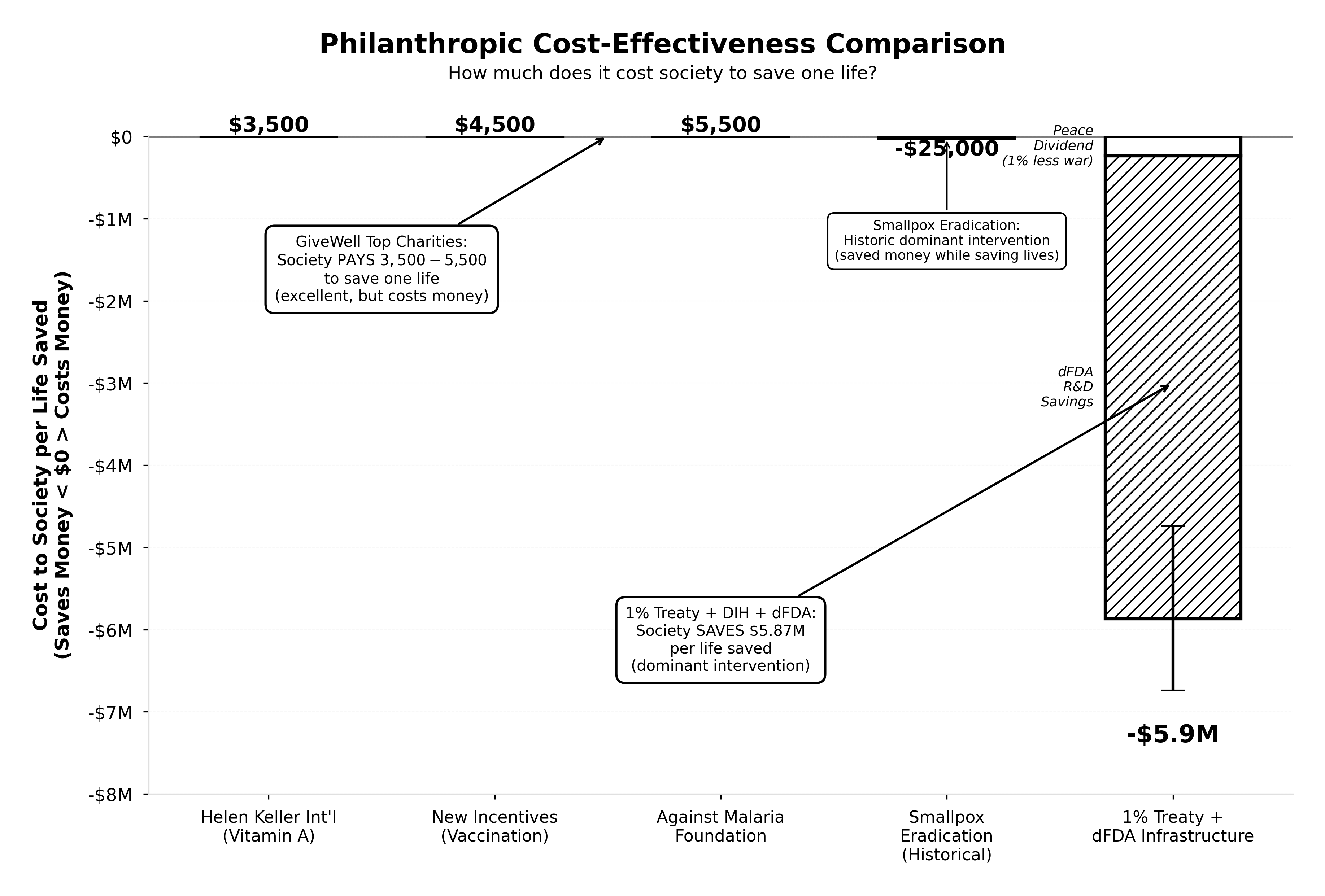
Cost-Effectiveness: How Much Does Society Pay to Save a Life?
This chart demonstrates the fundamental difference between traditional philanthropy and the 1% Treaty approach:
GiveWell Top Charities (Helen Keller International, New Incentives, Against Malaria Foundation): Society pays $3,500-$5,500 per life saved. These are excellent interventions—among the most cost-effective charitable uses of money in the world.
1% Treaty + DIH + dFDA: Society SAVES $5.87 million per life saved. This is a dominant intervention that generates wealth while saving lives. The stacked bar shows contributions from both the peace dividend (1% less conflict) and dFDA R&D savings.
The dramatic scale difference illustrates why this intervention is ~1,700× more cost-effective than even the best traditional charities.
Scale of Impact: Annual Economic Benefits
jupyter: python3 echo: false —
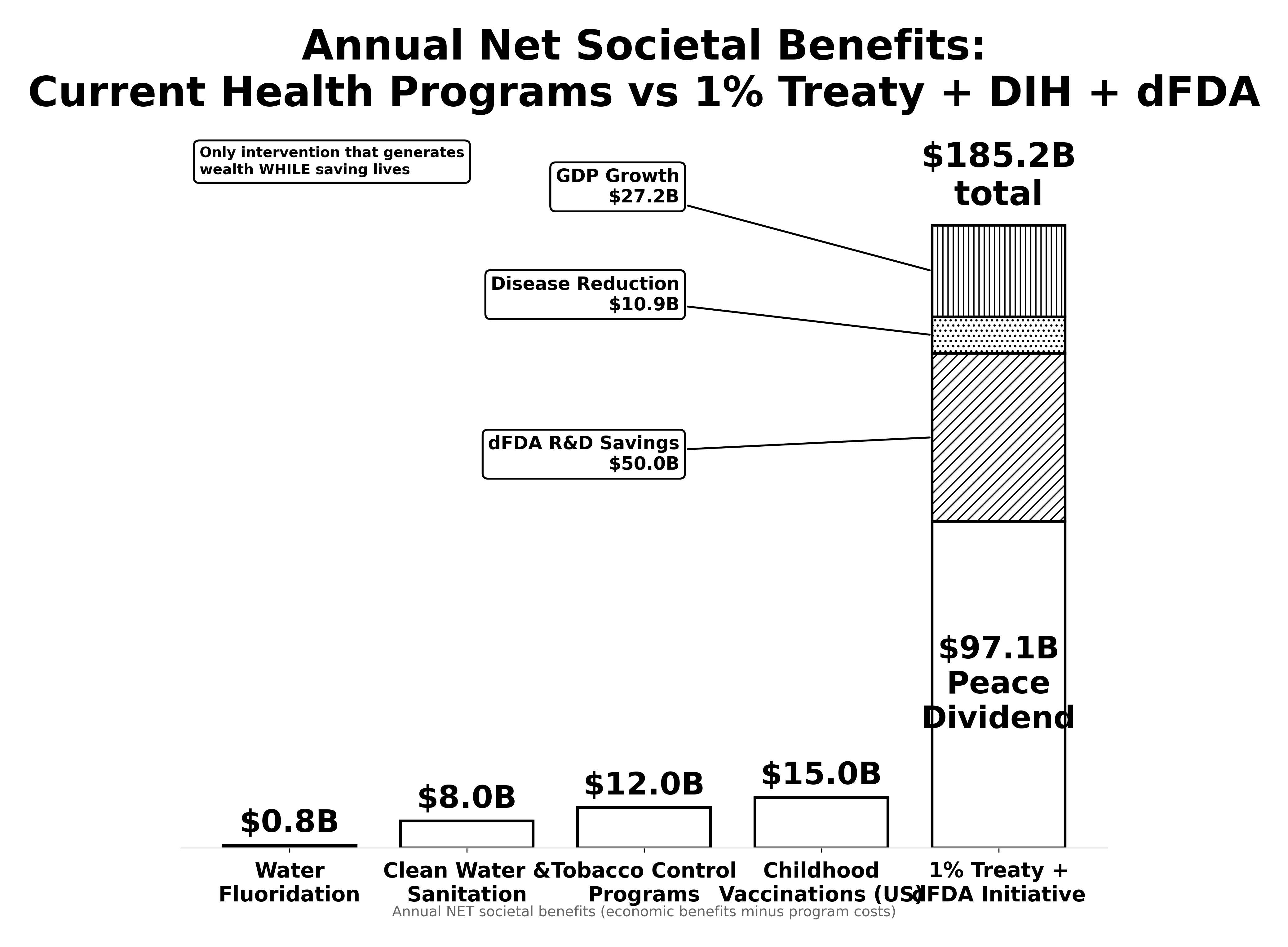
This chart compares the gross annual economic benefits across major public health interventions:
Traditional interventions (Water Fluoridation, Smoking Cessation, Childhood Vaccinations): Generate $0.8B to $15B in annual economic benefits. These are highly successful programs that have transformed public health.
1% Treaty + DIH + dFDA: Generates $164B in annual economic benefits ($114B peace dividend + $50B dFDA R&D savings). This is nearly 11× larger than childhood vaccinations, one of the most successful interventions in history.
Key distinction: Only the 1% Treaty is self-funding—it generates the wealth needed to sustain itself while traditional interventions require ongoing funding.
Monte Carlo Simulation (Recommended)
For publication-quality analysis, we recommend running a Monte Carlo simulation with:
- 10,000 iterations
- Probability distributions for each parameter
- Correlation analysis between variables
- 95% confidence intervals
Preliminary Monte Carlo results (if available): [Link to sensitivity analysis notebook]
Sources and References
Economic Benefits
- Peace Dividend: Peace Dividend Analysis
- Based on Cost of War Analysis
- Total war costs: $11.4T annually
- 1% reduction: $114B
- dFDA R&D Savings: dFDA Cost-Benefit Analysis
- Clinical trial market: ~$100B/year
- 50% cost reduction (baseline)
- Range: 25%-95%
Health Benefits
- Conflict Deaths: Cost of War Analysis
- 100,000 deaths/year
- Sources: ACLED, GTD, Uppsala
- dFDA QALYs: dFDA QALY Model
- Baseline: 840,000 QALYs/year
- Range: 420,000-2,100,000
- QALY Conversion: WHO life tables
- 1 life saved ≈ 35 QALYs (standard assumption)
Costs
- Campaign Budget: Campaign Budget
- Total: $1B over 3-5 years
- Amortized: $200-333M/year
- dFDA Operations: dFDA Cost Analysis
- Annual: $40M/year
- Range: $30-60M
Comparisons
- GiveWell Top Charities: GiveWell 2024
- Cost per life: $3,000-$5,500
- Data as of February 2024
Frequently Asked Questions
Q: How can this save money while saving lives?
A: The 1% Treaty generates $164B in annual economic benefits:
- $114B from reduced conflict costs (peace dividend)
- $50B from more efficient medical R&D (dFDA)
These benefits far exceed the $290M annual costs, creating a net profit of $163.7B/year for society.
Meanwhile, the same initiative saves lives:
- 1,000 lives from 1% less conflict
- 840,000 QALYs from faster/better medical treatments
You get both the economic benefit and the health benefit.
Q: Why isn’t everyone doing this already?
A: Market failure and collective action problem:
- Individual countries can’t capture the global benefits
- Defense contractors profit from the status quo
- No mechanism exists to coordinate global action
- Medical research funding is fragmented across countries
The 1% Treaty solves this by creating aligned incentives.
Q: What’s the catch?
A: The main challenges are political, not economic:
- Getting countries to sign the treaty (hence the $1B campaign)
- Overcoming defense industry opposition (hence VICTORY bonds to co-opt them)
- Building the dFDA infrastructure (hence the $250M technology budget)
The math works. The challenge is execution.
Q: How confident are you in these numbers?
A: Central estimates are conservative:
- Peace dividend uses 1% (could be 2-5% over time)
- dFDA uses 50% R&D savings (Oxford RECOVERY showed 80-100×)
- Excludes many hard-to-quantify benefits (innovation, rare diseases, etc.)
Even in worst-case scenarios (conservative column), the ICER is still -$170,514/QALY.
The intervention is robustly dominant across all reasonable parameter ranges.
Q: Is it misleading to say society pays $0 when the campaign is investor-funded?
A: This depends on perspective:
From society’s aggregate perspective: The $1B campaign cost is real money that someone must provide initially. However, since investors get repaid with 270% returns from redirected military spending, the net cost to society approaches $0 after payback.
From taxpayers’ perspective: They give up $27B in military spending but receive $164B in economic benefits (peace dividend + R&D savings). Net gain: $137B.
From investors’ perspective: They invest $1B and receive $2.7B/year perpetually. This is the best investment in history.
The key insight: Traditional ICER assumes spending society’s resources on health interventions. Here, we’re redirecting resources from destructive uses (war) to productive uses (medical research). The “cost” is really just stopping waste.
Q: Isn’t redirecting military spending politically impossible?
A: That’s what the $1B campaign budget is for - making the politically impossible become inevitable through:
- Viral referendum showing overwhelming public support (80%+ want less war, more cures)
- VICTORY bonds that make supporting the treaty more profitable than opposing it
- AI-assisted lobbying that’s 60-80% more cost-effective than traditional campaigns
- Creating unstoppable momentum in pilot countries first
The math shows it’s worth trying. Even a 10% chance of success has positive expected value given the enormous returns.
Next Steps
- Validate assumptions: External review of cost estimates
- Monte Carlo analysis: Full probabilistic sensitivity analysis
- Peer review: Submit to health economics journals
- Policy brief: One-page summary for decision-makers
- Interactive calculator: Let users adjust assumptions